Bridging the gap between healthcare service and agricultural productivity: pathway for rural development in Nigeria
Abstract
Agriculture remains a fundamental pillar of Nigeria’s economy, with rural households heavily reliant on farming for sustenance and income. However, poor health outcomes and limited access to healthcare services significantly hinder agricultural productivity. This study investigates the synergy between access to healthcare services and agricultural productivity among farming households in Nigeria. A multistage sampling technique was adopted to select 720 farming households in Southwest, Nigeria. Using a two-stage least squares (2SLS) regression model, the study examines how access to healthcare services influences farm productivity, employing distance to healthcare facilities as an instrumental variable. The findings reveal that farmers who utilize healthcare services exhibit higher productivity levels than those who do not. Specifically, the treatment group (households accessing healthcare services) reported a significantly higher value of farm produce sales (₦141,775.90) compared to the control group (₦102,430.11). Notable, major determinants of agricultural productivity include farm size, farming experience, cooperative membership, and access to health extension services, while distance to healthcare facilities negatively impacts healthcare utilization. The study highlights that frequent health-related incapacitation leads to labour loss and reduced efficiency, reinforcing the importance of an integrated approach to health and agriculture. Policy interventions such as mobile health clinics, community-based health insurance, and agricultural-health synergies could mitigate the adverse effects of poor health on agricultural output. Bridging the healthcare-agriculture divide is imperative for sustainable economic growth, improved food security, and poverty reduction in Nigeria.
Introduction
In sub-Saharan Africa, agriculture is the predominant economic activity, with more than half of the population engaged directly or indirectly (FAO, 2021; Omotoso et al., 2023). It employs more than 60% of the economically active labour force and contributes nearly 40% to total productivity in the Nigerian economy (Omotoso & Omotayo, 2024b; Outhwaite et al., 2022). Consequently, growth in agricultural productivity is essential for improving welfare, especially among rural households and achieving sustainable economic growth for poverty reduction (Outhwaite et al., 2022). It is noted that no country has been able to sustain a rapid transition out of hunger and poverty without raising productivity in its agricultural sector (Ali & Awade, 2019; Mirzabaev et al., 2023). Notably, agricultural productivity in Nigeria is dependent on physical strength and stamina, and therefore, health shocks are more likely to directly and indirectly affect workers’ productivity (Outhwaite et al., 2022).
Directly, ill health affects physical strength and work days/hours available for farm work while indirectly, ill health involving high medical expenditures tends to deprive farming households of resources to invest in experimentation on improved practices and the adoption of new technology (Gebrehiwot, 2015; WHO, 2023). Notably, poor health reduces farmers’ ability to innovate, experiment, and operationalize changes in agricultural systems (Omotoso & Omotayo, 2024c; Outhwaite et al., 2022). Serious health conditions resulting in catastrophic expenditures may also result in the depletion of productive assets such as the sale of draught animals and the sale of cultivable land (Outhwaite et al., 2022). The consequences of these actions include a reduction in farm sizes, cultivation of less-intensive crops, and reduction in livestock numbers resulting in poor livelihoods (WHO, 2021). The intersection of healthcare services, agricultural productivity, and rural development is critical to fostering sustainable economic growth and improving the well-being of rural populations (Bazzana et al., 2022).
In Nigeria, majority of rural households depend on agriculture for their livelihoods, yet they face significant health challenges that hinder productivity (Fadare et al., 2023; Gebrehiwot, 2015). Poor access to quality healthcare services, high disease prevalence, and inadequate health infrastructure reduce the labour efficiency of farmers, ultimately affecting agricultural output and rural development (Outhwaite et al., 2022; WHO, 2019). The health-capital transition, which refers to the shift in economic productivity due to improved health conditions, is essential for breaking the cycle of poverty and underdevelopment in rural areas where agriculture remains the backbone of the economy, contributing significantly to employment and food security (Combary & Traore, 2021; Liu et al., 2024). However, poor health conditions among farmers, including malnutrition, waterborne diseases, and occupational hazards, lead to reduced labour productivity and lower farm yields (Liu et al., 2024; Sabasi & Shumway, 2018). Without proper healthcare services, rural communities struggle with high morbidity rates, limiting their ability to engage in productive agricultural activities (Allen et al., 2014; FAO, 2021).
Despite extensive research on the individual aspects of healthcare services, agricultural productivity, and rural development, there remains a significant gap in understanding how these three domains intersect to drive economic transformation in Nigeria. Existing studies (Combary & Traore, 2021; Fink & Masiye, 2015) have primarily focused on the health-productivity nexus, emphasizing how poor health conditions reduce labour efficiency in agriculture. However, there is limited empirical evidence on how integrated healthcare and agricultural policies can create a sustainable health-capital transition in rural communities. Additionally, most studies (Mirzabaev et al., 2023; Sabasi & Shumway, 2018) on agriculture and rural development tend to overlook the critical role of healthcare services in enhancing farmers’ productivity and resilience. The link between rural health interventions and agricultural performance remains underexplored, particularly in the Nigerian context, where rural communities face both poor healthcare access and low agricultural yields.
Furthermore, there is a lack of comprehensive studies that analyze policy frameworks addressing the simultaneous improvement of healthcare infrastructure and agricultural productivity in Nigeria. While various government initiatives aim to boost agricultural development, there is little integration of healthcare policies that address the well-being of the farming population. Bridging the gap between healthcare and agricultural productivity requires a holistic approach that integrates health interventions, agricultural innovations, and rural development policies. Investments in rural health facilities, mobile health services, and agricultural extension programs can enhance farmers' well-being and improve their economic resilience. Additionally, strengthening health education, nutrition programs, and access to affordable healthcare services will ensure that rural populations remain healthy enough to sustain agricultural production.
Synergy between access to healthcare service and agriculture productivity
The interdependence between healthcare access and agricultural productivity is a crucial but often overlooked aspect of rural development. Agriculture remains the backbone of Nigeria’s economy, employing a significant portion of the rural population (Allen & Ulimwengu, 2015; Mirzabaev et al., 2023). However, agricultural productivity is highly dependent on the health status of farming communities, thus the ability of farmers to engage in physically demanding agricultural activities is directly influenced by their access to quality healthcare services (Combary & Traore, 2021; Gebrehiwot, 2015). Poor health conditions lead to reduced labour availability, lower efficiency, and ultimately, decreased agricultural output (FAO, 2021; WHO, 2021). A well-functioning healthcare system, therefore, enhances agricultural productivity by ensuring that farmers remain physically fit, reducing the burden of disease, and minimizing work disruptions due to illness (Allen & Ulimwengu, 2015; Fink & Masiye, 2015).
Interestingly, healthcare access in rural Nigeria is often constrained by inadequate infrastructure, long distances to health facilities, and financial barriers (Otekunrin et al., 2021; Oyekale, 2017). These challenges contribute to high rates of preventable diseases such as malaria, respiratory infections, and waterborne illnesses, which significantly reduce agricultural labour efficiency (Balogun, 2021). Studies (Allen & Ulimwengu, 2015; Fink & Masiye, 2015) have shown that health shocks, including chronic illnesses and malnutrition, lead to substantial losses in farm productivity. Additionally, (Kehinde et al., 2021; Liu et al., 2024) found that malaria prevalence and poor healthcare access among rural farmers in Northern Nigeria resulted in lower technical efficiency and reduced agricultural output. Similarly, (Kehinde et al., 2021; Oloruntoba et al., 2021) revealed that a single day of illness and inadequacy of healthcare access among agricultural workers in Southwest, Nigeria led to a full day or more of labour loss. These findings underscore the need for improved healthcare accessibility to sustain agricultural livelihoods.
Conversely, well-nourished farmers are less susceptible to diseases and can sustain higher levels of productivity (Oloruntoba et al., 2021). However, the absence of comprehensive healthcare interventions in rural areas exacerbates the vulnerability of farming households to health-related shocks (Bazzana et al., 2022; Chaud et al., 2021). Governments and policymakers have yet to fully integrate healthcare considerations into agricultural policies, resulting in fragmented development efforts (Daud et al., 2018; Mirzabaev et al., 2023).
To enhance the synergy between healthcare access and agricultural productivity, a multi-sectoral approach is needed. Policy interventions should include expanding rural healthcare infrastructure, subsidizing health insurance for farmers, and integrating health services into agricultural extension programs. By addressing healthcare challenges within the agricultural sector, Nigeria can achieve sustainable rural development, improved food security, and enhanced economic growth.
Material and Methods
Study area
The study was carried out in rural Southwest Nigeria, encompassing the states of Osun, Ogun, Ekiti, Ondo, Lagos, and Oyo. Agriculture is the primary livelihood activity in the geopolitical zone, with commercial production of maize, cassava, yam, oil palm, cocoa, and timber. The predominant households in this area depend mostly on subsistence farming, supplemented by income from trading, hunting, foraging, and handicrafts (Omotoso & Omotayo, 2024a). Consequently, rural households descended into a more acute poverty classification, compelling them to depend on savings and assistance from friends and relatives. The natural vegetation of the geopolitical zone consists of tropical rainforest in the south and guinea savannah in the north, with soil conducive to subsistence cultivation.
Sampling Procedures and Data Analysis
The study utilized primary data collected through an interview schedule. The study population is composed of rural farm households in the zone who primarily engage in subsistence farming. Additionally, 480 agricultural households across six (6) states in Southwestern, Nigeria were conducted using a multistage sampling procedure. The initial phase involved the deliberate selection of Ekiti, Ogun, and Oyo from the states that comprised the southwest geopolitical zone of Nigeria. The three states were selected due to their prominence in small-scale agricultural cultivation and their status as the food hub of the geopolitical zone. The second stage entails the selection of three zones from each state, resulting in a total of nine zones. In the third stage, a total of 2 blocks were randomly selected from nine zones in the area (18 blocks). In the fourth stage, four cells from each of the 18 blocks (a total of 72 cells) were randomly selected. The final stage entails the random selection of 10 rural farming households from each of the cells.
Consequently, a sample size of 720 rural farming households was employed in the study. Data about socio-economic characteristics, usage of health services, labour utilization patterns, and output value were gathered from the sampled households. The data were analyzed using descriptive statistics such as means, and standard deviation, two-sample t-test, and IV regression model. Ethical norms were rigorously followed. Before data collection, informed verbal consent was secured from each study participant, who were granted the complete right to withdraw from the interview at any point they felt uncomfortable. Moreover, secrecy was maintained by excluding the respondents' names from the data collection instrument, utilizing a unique identifying number as a code instead.
Model specification
Two stage least square (2SLS) selectivity model
Every impact assessment's primary focus is on treating non-compliers and removing selection bias (Bazzana et al., 2022). To address this, an instrumental variable model was used in the study. We can address the issue of treatment endogeneity and remove selection bias by using the conventional instrumental variables approach (Fink & Masiye, 2015). After controlling for observable characteristics, the technique implies the existence of at least one instrumental variable that explains the treatment but has no direct impact on the outcome. In order to account for any selection bias, we first calculated the following in light of the likely link between the decision to use health facilities and the observed or unobserved characteristics:
T = α0 + αiZi + δXi + µi ----------------------------(1)
Where;
Zi = represents the instrumental variable,
α0,αi and δi are parameter estimated
Following (Combary, 2016; Omotoso & Omotayo, 2024b), assessing the impacts of access to healthcare service on farm productivity, the second stage of the model is expressed as:
Ypt = β0 + βiTi + γXi + δi ----------------------------(2)
Where
Ypt = Agricultural productivity
Ti = represents the treatment variable taking the value of 1 for treated household and 0 otherwise
Xi = vector of control variables
Noteworthy, the treatment variable differentiates between households that use healthcare services when sick (yes = 1) and those that do not (no = 0), allowing for a comparative analysis of the impact of access to healthcare service on productivity. Following (Bazzana et al., 2022; Combary & Traore, 2021), to address potential endogeneity, distance to healthcare facilities is used as an instrumental variable, as it influences healthcare service access and utilization but does not directly determine farm productivity.
Results and Discussion
Description of variable used in the analysis
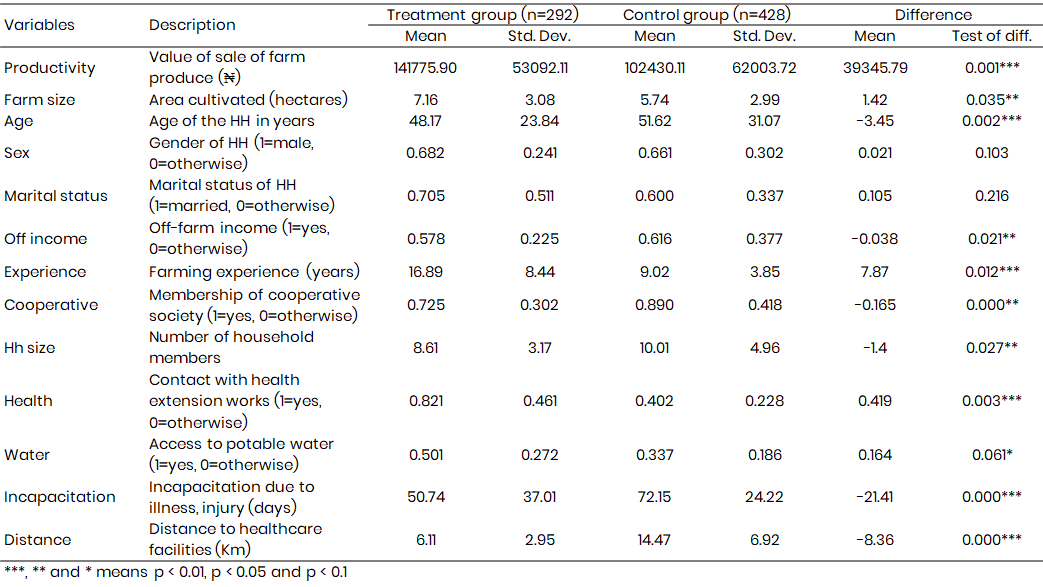
The findings from Table 1 underscore the significance of healthcare access in shaping the agricultural productivity and socioeconomic well-being of farming households. The treatment group - comprising households that accessed healthcare facilities - exhibited significantly higher agricultural productivity (₦141,775.90) compared to the control group (₦102,430.11), with a mean difference of ₦39,345.79 (p<0.001). This suggests that improved health conditions, facilitated by healthcare access, enhance the efficiency and productivity of farm labour. Healthier farmers are more capable of performing labour-intensive activities, thereby improving yields and farm income (Combary, 2016; Daud et al., 2018). The observed difference aligns with prior studies (Allen & Ulimwengu, 2015; Combary & Traore, 2021), which emphasize the role of health in ensuring a stable and productive agricultural workforce.
Consistently, farm size also varied significantly between the two groups, with the treatment group cultivating an average of 7.16 hectares compared to 5.74 hectares in the control group. Admittedly, larger farm sizes often require greater physical labour, which may be more effectively managed by healthier households with fewer incapacitating illnesses. Additionally, the treatment group had longer farming experience (16.89 years) than the control group (9.02 years), implying that households that prioritize health may have better agricultural knowledge and resilience against productivity shocks. Access to healthcare services was also associated with a higher likelihood of engagement with agricultural extension health services, cooperative membership and access to potable water suggesting broader positive spillover effects (Balogun, 2021).
Conversely, the control group reported a significantly greater average distance to healthcare facilities, reinforcing the role of physical accessibility in determining healthcare service accessibility. The control group also experienced higher days of incapacitation due to illness (50.74 days) compared to the treatment group which might indicate underreporting of illness or reliance on traditional healing methods rather than formal healthcare.
Furthermore, off-farm income engagement was slightly higher in the control group, possibly reflecting a coping strategy for households unable to maintain full agricultural labour due to untreated health issues (Oloruntoba et al., 2021). These results emphasize the critical interplay between health and labour efficiency in agricultural systems. Investing in healthcare infrastructure in rural farming communities could thus serve as a viable strategy for improving agricultural productivity and sustainable rural development.
Table 1: Variable description and descriptive statistic of treatment and control group (n=720)
Healthcare access and agricultural productivity – Two stage least squares estimation
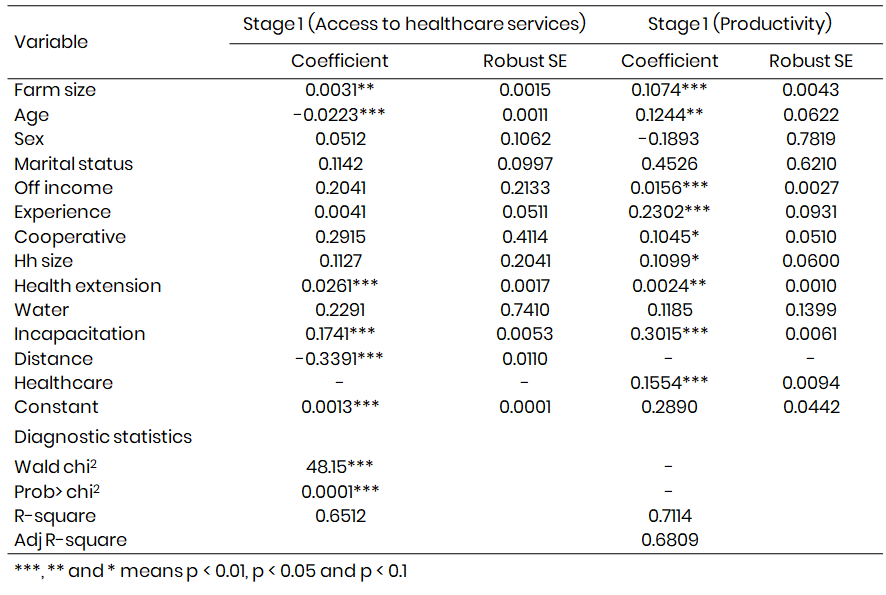
The results presented in Table 2 from Two-Stage Least Squares (2SLS) regression estimate highlight the determinants of healthcare access among farming households and the impact of healthcare access on agricultural productivity. The first stage of the regression estimates the likelihood of accessing healthcare services, while the second stage examines how healthcare access influences productivity. The findings from 2SLS regression provide compelling evidence on the link between healthcare access and agricultural productivity.
Stage 1 – Determinants of access to healthcare services
The first-stage 2SLS regression identifies key factors influencing access to healthcare services among farming households. The significant and negative effect of distance to healthcare facilities (β = -0.3391, p < 0.01) corroborates previous studies (Allen & Ulimwengu, 2015; Combary, 2016) that have highlighted distance as a major barrier to healthcare utilization in rural settings. Long distances increase travel costs and reduce the likelihood of timely medical attention, leading to worsening health conditions (Combary & Traore, 2021).
Furthermore, the positive effect of access to health extension workers (β = 0.0261, p < 0.01) on healthcare access is consistent with (Oyekale, 2017; Rufai et al., 2021), who emphasized the role of community-based health interventions in improving healthcare utilization. The role of incapacitation due to illness (β = 0.1741, p < 0.01) is also notable, suggesting that severe health challenges push households to seek medical attention. Interestingly, age (β = -0.0223, p < 0.01) negatively affects healthcare access, a result that supports previous studies (Otekunrin, 2022; Rutledge et al., 2023) indicating that older individuals, particularly in rural areas, may face mobility and financial constraints when seeking medical care.
Stage 2 – Effect of healthcare service access on agricultural productivity
The second-stage regression establishes a significant positive relationship between healthcare access (β = 0.1554, p < 0.01) and agricultural productivity, reinforcing the argument that health is a critical determinant of labour efficiency and farm productivity. Farmers who utilize healthcare services are more productive, as they experience fewer workdays lost to illness and maintain higher energy levels to perform physically demanding agricultural activities (Rutledge et al., 2023; WHO, 2021). This finding aligns with studies by (Liu et al., 2024; Oloruntoba et al., 2021), who reported that health investments significantly enhance labor productivity and agricultural output.
Moreover, incapacitation due to illness (β = -0.3015, p < 0.01) significantly reduces productivity, highlighting the negative economic consequences of poor health in rural areas. This finding resonates with (Otekunrin, 2022; WHO, 2021), who demonstrated that malaria prevalence among farmers in Northern Nigeria led to reduced farm output and technical efficiency. The impact of health-related labor losses was also documented by (Omotoso & Omotayo, 2024b; Otekunrin, 2022), who found that each day of illness among agricultural workers resulted in more than a day of lost labour. Other productivity-enhancing factors identified include farm size (β = 0.1074, p < 0.01) and farming experience (β = 0.2302, p < 0.01), both of which have been widely acknowledged in agricultural economic literature as critical determinants of farm efficiency (Kehinde et al., 2021; Liu et al., 2024).
The positive role of cooperative membership (β = 0.1045, p < 0.1) and household size (β = 0.1099, p < 0.1) suggests that access to social capital and a larger labour pool improve farm productivity. Noteworthy, significant evidence supporting the positive impact of healthcare access on agricultural productivity suggests the need for rural health policy interventions that reduce barriers to healthcare utilization. The findings reinforce the bidirectional relationship between health and agriculture. Strengthening healthcare access not only enhances individual well-being but also serves as a key driver of rural economic development, supporting Nigeria’s broader goals of food security and poverty reduction (Allen et al., 2014; Allen & Ulimwengu, 2015; Daud et al., 2018)
Table 2: Instrumental variable – Two stage least square regression estimate (n=720)
Conclusion
Access to healthcare services is essential for maintaining a healthy workforce, yet many rural farmers face challenges such as long distances to healthcare facilities, high costs, and inadequate medical infrastructure. This study examines the impact of access to healthcare services on agricultural productivity among farming households in Nigeria. Using the Instrumental Variable Two-Stage Least Squares (2SLS) regression approach, the findings reveal that households with better healthcare access exhibit higher agricultural productivity compared to those that do not seek medical care. Distance to healthcare facilities is a major determinant of healthcare utilization, negatively impacting farm productivity due to increased health-related incapacitation.
The results underscore the critical role of healthcare in enhancing agricultural labor efficiency, reinforcing the argument that poor health is a major constraint to rural development and food security. Key factors influencing healthcare access include proximity to health facilities, health extension services, farm size, and off-farm income. Productivity is significantly driven by farm size, farming experience, cooperative membership, and household size, emphasizing the need for economic and social resources to enhance agricultural outcomes. Health-related incapacitation negatively affects productivity, highlighting the economic burden of untreated illnesses on farming households.
The study recommends expanding rural healthcare infrastructure, strengthening health extension services, and implementing affordable health insurance schemes for farmers. Integrating health interventions into agricultural policies is essential for achieving sustainable food security and rural development.
Acknowledgements
The authors acknowledge and appreciate Tertiary Education Trust Fund (TetFund) Institutional Based Research (IBR) for the financial and technical support towards the success of this research. Additionally, the conducive environment support by Oyo State College of Agriculture and Technology, Igboora, Nigeria for the successful completion of this research work is appreciated and recognized. Opinions and conclusions herewith are those of the authors and are not necessarily to be attributed to the bodies.
Data availability
The data underlying this article will be shared on reasonable request from the corresponding author.
References
Ali, E., & Awade, N. E. (2019). Credit constraints and soybean farmers' welfare in subsistence agriculture in Togo. Heliyon, 5(4).
Allen, S., Badiane, O., Sene, L., & Ulimwengu, J. (2014). Government expenditures, health outcomes and marginal productivity of agricultural inputs: the case of Tanzania. Journal of Agricultural Economics, 65(3), 637-662.
Allen, S. L., & Ulimwengu, J. (2015). Agricultural productivity, health and public expenditures in Sub-Saharan Africa. The European Journal of Development Research, 27(3), 425-437.
Balogun, J. A. (2021). Nigerian Healthcare System. Springer.
Bazzana, D., Foltz, J., & Zhang, Y. (2022). Impact of climate smart agriculture on food security: An agent-based analysis. Food Policy, 111, 102304.
Copyright
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.

